
Real-time EMR sync is no longer a future goal. It sits in the middle of your clinical workflow, your quality metrics, and your patient experience today. You feel it any time clinicians log into three systems to piece together a single patient story. Or when your revenue cycle slows because encounters exist in one EMR and not another.
You do not fix that with one more point-to-point interface. You fix it with a clear healthcare IT roadmap, purpose-built for real-time EMR sync, supported by the right integration partner.
This guide gives you a practical path. You will see what to prioritize, how to structure your architecture, and where real risk hides, so you can move from fragmented interfaces to true clinical data exchange at scale.
Why Real-Time Sync Matters
Clinical impact you can measure
When your systems lag, your care teams work blind. Orders entered in one EMR do not show in another until a nightly batch. Allergy updates in the ambulatory record never reach the hospital chart in time.
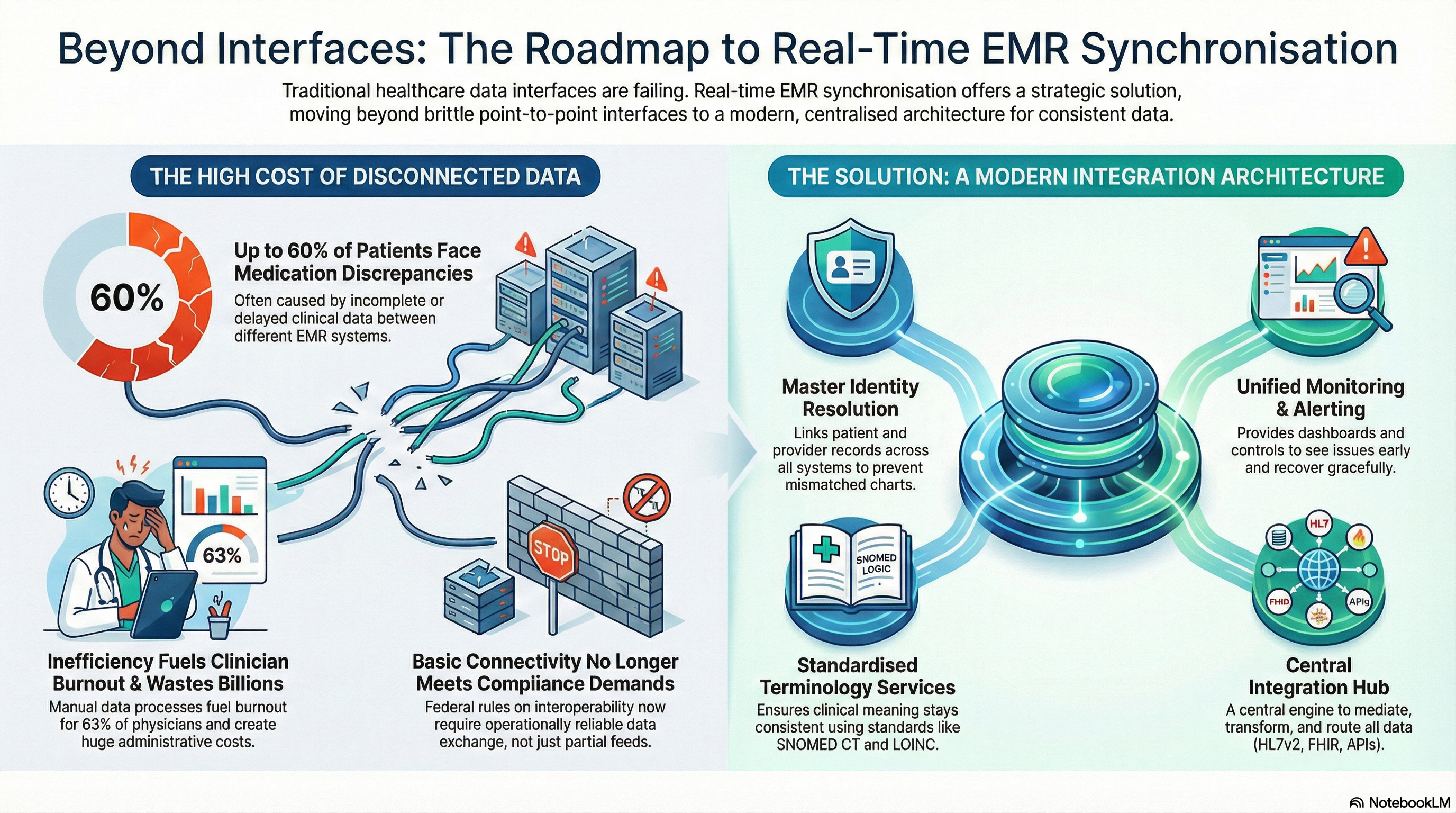
Real-time EMR sync closes those gaps. It keeps orders, results, problems, and meds aligned across EMRs as soon as events occur. That shift directly affects outcomes and safety. A large review of medication histories found that reconciliation discrepancies affect between 14 percent and 60 percent of patients in some settings, often due to incomplete data in source systems. When your systems share the same current record, you lower the risk of conflicting orders and duplicate therapies.
Operational and financial value
Real-time EMR sync also hits operations and margins. Manual chart chasing, duplicate registration, and claim edits all cost staff time and delay revenue. In one study, hospitals spent about $39 billion per year on administrative complexity tied to manual and nonstandard processes. When data flows cleanly and quickly, you cut manual work and reduce rework in both clinical and back office teams.
Real-time EMR sync helps your clinicians too. A national survey found that 63 percent of physicians reported burnout drivers related to documentation and technology burden. Each workflow you simplify with reliable clinical data exchange pulls some pressure off your teams.
Regulatory and ecosystem pressure
EMR interoperability is no longer optional. Federal rules on information blocking and interoperability push you toward better clinical data exchange with payers, HIEs, and other providers. ONC has reported that by 2021 about 88 percent of hospitals were electronically exchanging health information with outside providers, but many still rely on partial and delayed feeds.
Real-time EMR sync moves you from “technically connected” to “operationally reliable.” That difference matters when auditors review your interoperability posture or when executives ask why readmissions and leakage still sit above target even with interfaces in place.
Architecture Overview
Key building blocks
Effective healthcare data synchronization architecture respects both your current EMRs and your long term roadmap. You do not rip and replace. You interpose a stable, intelligent integration layer that coordinates data, security, and monitoring across systems.
At a minimum, your real-time EMR sync architecture should include:
• Integration hub or interoperability platform A central engine that handles HL7v2, FHIR, proprietary APIs, and file-based events. This hub mediates, transforms, and routes messages for all clinical data exchange.
• Event streaming backbone A message queue or streaming platform that moves events in near real time. This avoids lockstep dependencies between EMRs and allows scale.
• Master patient index and provider registry Identity resolution aligns patients and providers across systems. Without this, real-time EMR sync only spreads mismatched charts faster.
• Terminology and mapping services Standardization across vocabularies such as LOINC, SNOMED CT, and RxNorm. This keeps clinical meaning consistent from source to target.
• Monitoring, alerting, and replay tools Operational dashboards, exception queues, and replay controls so your team sees issues early and recovers gracefully.
Event driven, not only request driven
Many organizations start with point-to-point APIs that answer “pull” requests. Real-time EMR sync needs an event driven model. Source systems emit events on change. Subscribers listen and act.
This pattern supports:
• Updates across any number of EMRs for a single event.
• Downstream analytics and population health tools that listen to the same stream.
• More resilient behavior when one target system goes offline.
Logical flow for real-time EMR sync
A typical flow for healthcare data synchronization looks like this:
• Event occurs in the source EMR, such as admit, discharge, lab result, or medication update.
• Source posts a message to the integration hub using HL7, FHIR, or API.
• Hub validates, enriches, and maps data to standard structures.
• Identity services link the event to a unified patient and provider record.
• Routing rules send the event to target EMRs and other subscribed systems.
• Targets acknowledge, store, and surface the data in clinical workflows.
• Monitoring logs the transaction and raises alerts on errors or delays.
With an architecture like this, you gain a controllable middle layer instead of many brittle custom interfaces.
Implementation Roadmap
1. Define scope and success metrics
Start with a narrow, high value scope for real-time EMR sync.
• Decide which EMRs and systems participate in phase one.
• Specify data domains: ADT, orders, results, meds, allergies, problems.
• Set clear service level targets, such as “95 percent of messages processed in under 5 seconds.”
• Agree on success measures, for example fewer duplicate tests, faster discharge summaries, fewer chart corrections.
Align these outcomes with your broader healthcare IT roadmap, not just with a single project.
2. Assess current interfaces and gaps
Inventory existing HL7 feeds, FHIR APIs, and flat file processes. Note message types, volumes, schedules, and failure patterns.
For each participating EMR, document:
• Supported integration standards and versions.
• Current identity management approach and any local MRN rules.
• Configuration limits affecting real-time activity, such as throttling and batching.
• Monitoring coverage and who owns support today.
This assessment often surfaces overlapping feeds and brittle custom scripts, both of which slow true EMR interoperability.
3. Design your canonical data model and routing rules
Define a canonical representation of core objects: patient, encounter, order, result, medication, provider. Map each EMR’s data structures to this model.
Then define routing and transformation rules:
• Which events must sync, and which stay local.
• Which system serves as source of truth for each domain.
• How to handle conflicts when two systems update the same element.
• When to aggregate or split messages for downstream systems.
Investing in this design stage helps you avoid ad hoc decisions during testing and go live.
4. Build and configure the integration platform
With scope and design in place, you configure your integration layer. Actions here include:
• Standing up connection endpoints for each EMR and ancillary system.
• Implementing transformations between HL7v2, FHIR resources, and internal formats.
• Integrating an MPI or patient matching service for cross-system identity resolution.
• Implementing terminology mapping so codes remain consistent across targets.
• Configuring queues, retry logic, and back pressure controls for traffic spikes.
During this phase, concise logging and correlation IDs for each message become essential. Your team needs traceability to support clinicians when questions arise.
5. Establish governance and change control
Real-time EMR sync touches multiple vendor contracts, compliance obligations, and clinical workflows. You need a governance model that can make decisions quickly and keep stakeholders aligned.
Build a cross functional group with:
• Clinical leaders from key service lines.
• IT integration and security leaders.
• Compliance and privacy officers.
• Revenue cycle and operations leadership.
Define clear change control. Minor interface updates should follow a light path. Structural changes, such as new data domains or new EMRs, use a more formal review. This structure helps you scale your healthcare IT roadmap over several years without chaos.
6. Test with clinical workflows, not only with test harnesses
Pure technical testing finds parse errors and throughput issues, but it misses workflow misalignment. Include clinicians early.
For each workflow, such as ED arrival, admission, order entry, and discharge, walk through:
• Where the event starts and which EMR is primary.
• What each downstream EMR should show, when, and in which view.
• How updates and corrections behave and how staff see status.
• How downtime procedures work when one system is offline.
Capture issues such as duplicate orders, confusing flags, or delayed visibility, and refine your routing and display logic.
7. Roll out in phases with strong support
Start with one region, service line, or EMR pair. Provide clear training and short playbooks for support teams.
In the first weeks after go live, track:
• Message volumes and latency against your targets.
• Error rates and root causes.
• Clinician feedback, especially any patient safety concerns.
• Operational metrics, such as reduced duplicate tests or fewer manual chart merges.
Use this feedback loop to tune performance before you expand to more systems and facilities.
Security Considerations
Protecting PHI across every hop
Real-time EMR sync increases the number of systems and services that touch protected health information. Your security model must treat the integration layer as a first class clinical system, not as plumbing.
Key controls include:
• Encryption in transit and at rest All traffic between EMRs, integration hubs, and downstream systems should use strong TLS. Store logs and queues in encrypted form.
• Strong identity and access management Use service accounts with least privilege, with clear ownership and rotation policies. Tie human access to role based controls and centralized directories.
• Segmentation and network controls Separate integration subnets, restrict inbound paths, and control management interfaces tightly.
Auditability and compliance
Every data movement across EMRs should leave an auditable trail. When clinicians raise questions or when auditors review your controls, you need quick, clear answers.
Effective real-time EMR sync platforms maintain:
• Comprehensive transaction logs with timestamps, source, target, and disposition.
• Configurable retention that aligns with your record keeping and legal needs.
• Dashboards that highlight potential breaches or unusual data movement patterns.
The U.S. Department of Health and Human Services reports that large healthcare data breaches affected more than 88 million individuals in 2023. Strong visibility and control in your integration layer reduces exposure and improves incident response if an issue occurs.
Vendor and third party risk
Your integration partner and related vendors sit inside your risk surface. Treat them as strategic security partners.
As you evaluate or manage partners, review:
• Independent certifications, such as SOC 2 or HITRUST, and their scope.
• Data residency and hosting arrangements.
• Support for modern authentication and authorization standards.
• Processes for security updates, vulnerability management, and incident communication.
Include your integration layer in annual risk assessments and tabletop exercises so you know how it behaves under stress.
Conclusion
Real-time EMR sync is a strategic capability. It supports safer care, leaner operations, and regulatory alignment. Yet it touches identity, terminology, workflow, and security, so it demands more than a few additional interfaces.
You need a clear healthcare IT roadmap, a strong integration architecture, and a partner that lives in the details of EMR interoperability. With those in place, you move from fragile point solutions to a stable foundation for every future digital initiative.
Vorro focuses on real-time healthcare data synchronization, clinical data exchange, and integration at scale. If you are ready to modernize your real-time EMR sync strategy, talk with Vorro about your integration roadmap.
FAQs
What is real-time EMR sync?
Real-time EMR sync is the continuous exchange and alignment of clinical and administrative data across multiple EMRs and related systems with minimal delay. Events in one system, such as admissions, orders, or results, propagate to others in seconds. This supports accurate, current information for clinicians and operations across your network.
How is real-time EMR sync different from traditional interfaces?
Traditional interfaces often rely on batch jobs and tightly coupled point-to-point connections. Real-time EMR sync uses an integration hub, standardized models, and event driven patterns. This design supports lower latency, higher resilience, and easier scaling to new systems and workflows.
Which data should you prioritize in early phases?
Start with high impact domains that affect safety and coordination. Typical first phase scopes include ADT events, medications, allergies, problem lists, orders, and results. You can then extend to documents, notes, and specialized registries as your platform stabilizes.
How long does a real-time EMR sync project usually take?
Timelines depend on the number of EMRs, current integration maturity, and scope. Many organizations see initial production use between six and twelve months after project start for a defined EMR pair and limited data set. Broader rollout happens in phases over several years as part of a structured healthcare IT roadmap.
What role does FHIR play in real-time EMR sync?
FHIR provides modern APIs and standard resource models for clinical data exchange. Many EMRs now expose FHIR endpoints that support more granular and flexible integration. A strong integration platform uses FHIR where available while also supporting HL7v2, proprietary APIs, and other formats so you can bridge new and legacy systems in one environment.
