
Every decision you make in care delivery depends on one thing first, knowing exactly which patient you are looking at. Patient identity matching sits at the center of that problem. When identity is wrong, every downstream step becomes risky. Orders, medications, referrals, billing, analytics, and population health all inherit the error.
You feel this risk growing as data flows between EHRs, HIEs, payers, labs, and digital front doors. More portals. More devices. More encounters. All pointing to the same person, or at least they should.
In this environment, patient identity matching is no longer an internal data task. It is a safety discipline, a regulatory expectation, and a strategic requirement for any organization that wants reliable analytics and coordinated care.
Identity Matching Challenges
Patient identity matching sounds simple. In practice, it is one of the hardest data problems in US healthcare.
Fragmented identifiers
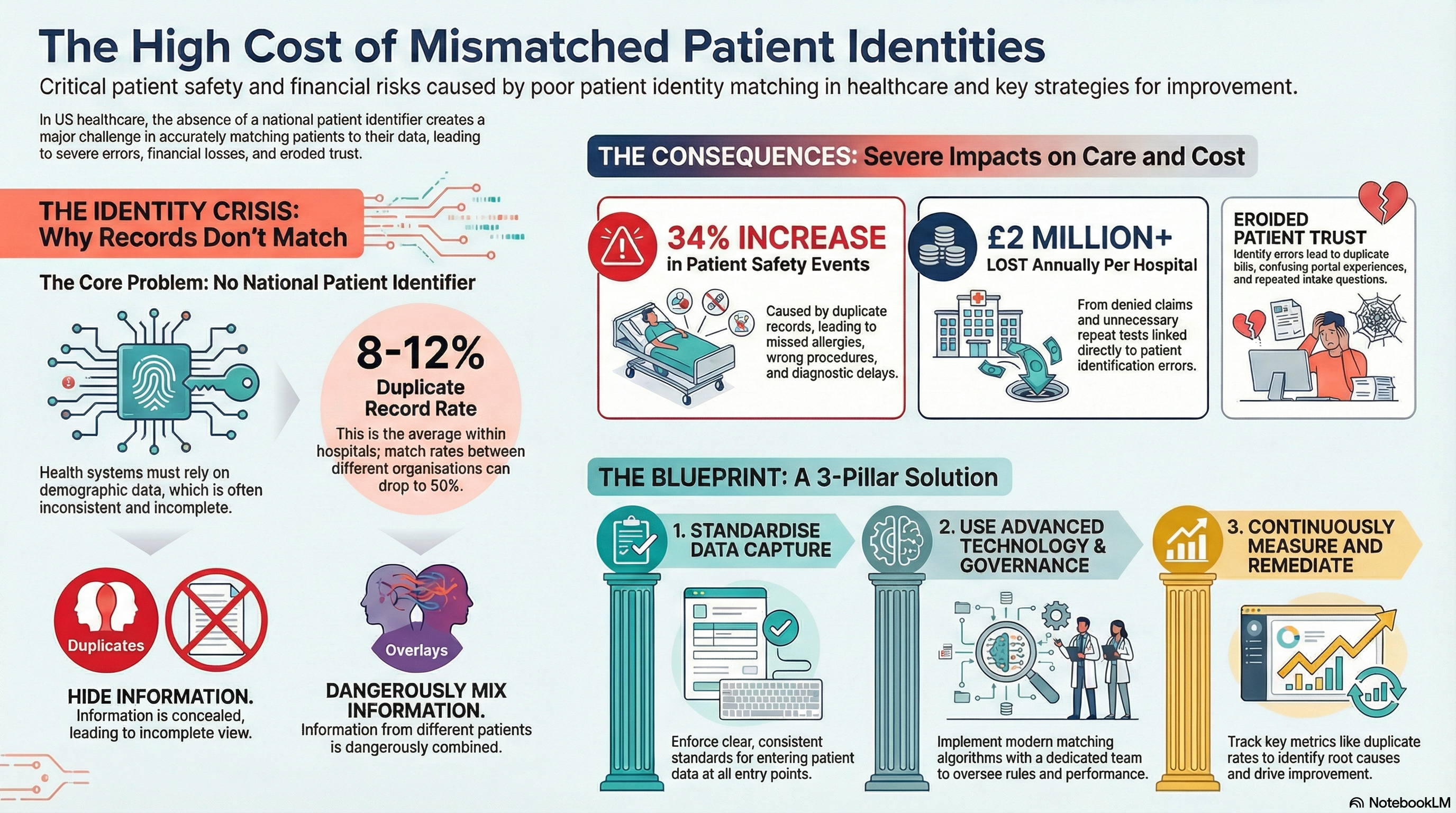
The lack of a national patient identifier in the United States creates a structural barrier. Every health system, HIE, and vendor uses its own set of identifiers to resolve identity across encounters and systems.
As a result, the average hospital carries a significant amount of duplicate and overlaid records. The American Hospital Association reported average duplicate record rates between 8 and 12 percent within organizations. Across organizations, match rates can drop to around 50 percent when data is shared.
Without a shared identifier, you rely on demographic fields, probabilistic algorithms, and manual review. Each carries its own weaknesses and costs.
Data quality and variability
Even before you match records, you face gaps and variation in the underlying data. Name formats differ. Addresses change. Phone numbers and emails expire. Patients use nicknames, middle names, married names, or alternate spellings.
Simple workflow decisions, like how front desk staff enter names or addresses, produce large swings in your match rates. One registration team might abbreviate “Street” and “Avenue.” Another might not. One team might verify date of birth at each visit. Another might skip that step.
Over time, these small differences accumulate into significant healthcare interoperability challenges. Every variation introduces uncertainty for an EMR patient matching algorithm that tries to determine if two records belong to the same person.
Interoperability at scale
As your data footprint grows, identity matching must scale with it. National networks intensify this challenge. CommonWell, Carequality, and TEFCA frameworks increase data liquidity, but they also expose how fragile identity resolution can be when systems interpret and format data differently.
ONC reported that patient match rates between organizations range from 50 to 60 percent in many exchange scenarios. That gap directly affects everything from medication reconciliation to value based care analytics.
Common Errors
Patient identity matching breaks down in a few consistent ways. Understanding these patterns helps you address the root causes.
Duplicate records
Duplicate records occur when your system creates a new MRN or profile for a patient who already exists in your database. Sometimes the patient presents with a slightly different name or address. Sometimes staff search incorrectly or face time pressure and opt to create a new record.
Duplicate rates as low as a few percent still lead to thousands of fragmented records across a large health system. One study found that duplicate records increased patient safety events by 34 percent compared with clean records. That risk compounds as you exchange data with external partners.
Overlays and mis‑merges
Overlays occur when information from two different people merges into a single record. This is one of the most serious identity failures because clinicians see a blended chart and often do not know it.
Mis merges can happen when manual staff or automated algorithms overconfidently merge two records based on partial matches. Shared address, similar name, or close date of birth might be enough to trigger a merge in a poorly tuned system.
AHIMA and CHIME have highlighted overlay rates between 1 to 3 percent in some organizations. Each overlay exposes patients to wrong medications, missed allergies, and billing errors that erode trust quickly.
Demographic drift
Patients move, change phone numbers, and update email addresses often. Without regular data stewardship, your registration data decays quickly. Some industry estimates show that contact data decays at a rate of about 10 to 20 percent each year.
When addresses, phone numbers, and emails go stale, both EMR patient matching algorithms and manual staff lose reliable anchors. You see more near matches, more manual queue volume, and more risk of missing a match that matters.
Best Practices
To improve patient identity matching, you need a coordinated approach across people, process, and technology. Technology alone will not solve identity if workflows and governance do not support it.
Standardize data capture at entry points
Start with how data enters your systems. Build clear, enforced standards for registration, scheduling, and digital front door workflows.
• Define required fields for every encounter. At minimum, use full legal name, date of birth, address, phone, and email.
• Establish standard formats for name, suffixes, addresses, and phone numbers.
• Use address verification tools aligned to USPS standards during registration.
• Train front line staff regularly and provide simple job aids.
Even small standardization steps can improve healthcare data accuracy across your ecosystem, reduce duplicate creation, and support more accurate downstream matching.
Use advanced matching algorithms with clear governance
Move beyond exact matching on a small set of fields. Probabilistic and referential matching techniques analyze more attributes and assign confidence scores that better reflect real world data variation.
Strong EMR patient matching programs combine:
• An enterprise master patient index or enterprise identity solution.
• Configurable matching rules tuned to your data profile.
• Thresholds for auto match, potential match, and non match outcomes.
• Clear workflows for manual review queues.
At the same time, you need formal governance. Define an identity stewardship team with the authority to set rules, monitor performance, and adjust configurations as your data sources change.
Continuously measure and remediate
Patient identity matching is not a one time project. It is an ongoing program that needs measurement and continuous improvement.
• Track duplicate creation rates by location, department, and user role.
• Monitor overlay incidents and root causes.
• Measure match rates for internal and external exchanges.
• Run periodic audits of high risk populations and workflows.
Health systems that addressed identity as a formal safety and quality initiative reported reduced duplicate rates of up to 30 to 40 percent after targeted interventions. That type of improvement requires consistent operational focus.
Integrate identity into interoperability strategy
You cannot treat identity as a local issue when your data increasingly flows through networks and partner systems. Identity work must sit inside your broader interoperability roadmap.
That includes:
• Aligning identity matching rules with your HIEs and major trading partners.
• Defining how you handle cross organizational patient record duplication.
• Using shared identifiers where available, such as HIE or network level IDs.
• Testing match performance and data quality before expanding new interfaces.
When you connect new EMR instances, labs, payers, or digital tools, identity matching should be a core part of go live criteria, not an afterthought.
Impact on Care
Patient identity matching is often framed as a data quality issue. In practice, it is a front line clinical safety issue and a key driver of financial and operational outcomes.
Patient safety and clinical quality
Duplicates and overlays change what a clinician sees at the point of care. Allergies, medication lists, problem lists, and lab results might be incomplete, wrong, or associated with another person.
The ECRI Institute identified patient identification errors as a top safety concern, contributing to wrong patient procedures and diagnostic delays in multiple settings. In one analysis of events in Pennsylvania, ECRI found that identification issues played a role in nearly 9 percent of reported errors related to lab and diagnostic testing.
Strong identity programs help clinicians trust what they see. That trust supports faster decisions, fewer repeat tests, and lower cognitive load in already stressed environments.
Financial performance and operational efficiency
Poor identity matching contributes to denied claims, rework, and unnecessary utilization. When two records for the same patient sit in different systems, your revenue cycle teams struggle to reconcile charges and coverage accurately.
A Ponemon Institute study estimated that healthcare organizations lose about $1.5 million per year on average due to⁸ denied claims linked to inaccurate patient identification and registration errors. The same study found an average of $1million per year in unnecessary repeat care, including imaging and lab tests, tied to identity and record matching issues.
Strong identity matching also improves your analytics. Population health, risk stratification, quality measure reporting, and value based care performance all depend on accurate longitudinal views. If one patient appears as three, every metric you calculate loses precision.
Patient experience and trust
From the patient perspective, identity errors feel personal. They lead to repeated intake questions, conflicting information, duplicate bills, and confusing portal experiences.
When patients receive care in multiple settings, they expect their information to follow them. Strong patient identity matching supports smoother digital experiences, consistent communication, and fewer frustrating surprises at check in or billing.
Conclusion
Patient identity matching sits at the foundation of safe, coordinated, data driven care. It shapes how you address healthcare interoperability challenges, how you maintain healthcare data accuracy, and how you control patient record duplication inside and outside your walls.
You strengthen identity matching when you:
• Standardize data capture for every encounter and channel.
• Adopt modern, governed matching technology tuned to your data.
• Measure performance continuously and address root causes.
• Integrate identity into every interoperability and integration decision.
This work is not only about protecting your data. It is about protecting your patients, supporting your clinicians, and giving your organization the confidence to share and use data at scale.
Vorro helps health systems, HIEs, and digital health organizations improve identity resolution as part of a broader integration and interoperability strategy. Our integration platform focuses on consistent, high quality data flow between systems so your clinical and analytics teams can rely on the identity layer that supports every decision.
If you are ready to strengthen your patient identity matching program and reduce interoperability friction, connect with Vorro and align your data foundation with your care and business goals.
FAQs
Why is patient identity matching so difficult in US healthcare?
The United States does not use a single national patient identifier, so organizations rely on local identifiers and demographic fields to match records. Data formats differ across EHRs, HIEs, and partners. Names, addresses, and contact details change over time. All of this creates ambiguity, which lowers match rates and increases both duplicates and overlays.
How does patient record duplication affect patient care?
Duplicate records fragment a patient’s history across multiple charts. Clinicians might not see all medications, allergies, or test results during an encounter. That gap increases the risk of missed information, repeat testing, and treatment delays. Duplicates also raise manual workload for registration, HIM, and revenue cycle teams, which can slow access and billing.
What is the difference between a duplicate record and an overlay?
A duplicate record occurs when the same person has more than one medical record in your system. An overlay occurs when information from two different people merges into one record. Duplicates hide information. Overlays mix information. Both are serious, but overlays present especially high clinical risk because clinicians might see data for the wrong person without realizing it.
How can technology improve EMR patient matching?
Advanced EMR patient matching tools use probabilistic and referential techniques to evaluate many data points instead of simple one to one field comparisons. They assign match scores, support configurable rules, and route ambiguous cases to manual review queues. When combined with strong data standards and governance, these tools significantly improve match rates inside organizations and across exchanges.
Where does Vorro fit into a patient identity strategy?
Vorro focuses on data integration across your ecosystem, which directly affects identity performance. We help you standardize and transform incoming data, align with partner systems, and maintain consistent identifiers across interfaces. That support gives your master patient index or identity tools cleaner, more reliable inputs, and reduces the identity friction that often slows interoperability projects.
